
Blue Cross Blue Shield of Arizona issued the following announcement on July 16
DOUBLE DIGIT INCREASES IN RISK FACTORS AMONG MILLENNIALS
While the overall rate of colorectal cancer diagnoses remained steady through 2018, the prevalence of conditions that increase the risk for colorectal cancer has increased dramatically. Crohn’s disease, ulcerative colitis, diabetes and diagnosed obesity are up significantly among some age groups, especially millennials. This trend among millennials significantly increases the risk of future diagnoses of colorectal cancer.
CHRONIC DISEASES INCREASE THE RISK FOR COLORECTAL CANCER
The American Cancer Society recognizes these chronic conditions increase the risk for colorectal cancer.5 Data from the Blue Cross Blue Shield (BCBS) Health Index6 show that patients with Crohn’s and ulcerative colitis are at a nearly twofold increased risk for colorectal cancer, and patients with diabetes or diagnosed obesity are at a 1.7 and 1.3 times greater risk of getting colorectal cancer, respectively, compared to those without these conditions
The 2019 Health of Millennials report found double digit increases among millennials for type II diabetes and Crohn’s and ulcerative colitis — prevalence rates significantly higher than in their Gen X counterparts at the same age.
COLORECTAL CANCER DIAGNOSES ARE HIGHER IN THE SOUTH AND NORTHEAST
The overall rate of colorectal cancer diagnoses among commercially insured Americans has remained largely steady across all age groups since 2014, at about 32.7 per 10,000 in 2018 or about 282,000 individuals for both men and women.
The prevalence of colorectal cancer is highest in parts of the South and Northeast U.S. (excluding New England). Rates of Crohn’s disease and ulcerative colitis follow a similar regional pattern with the highest rates in the South and Northeast (See Appendix). Rising rates of these conditions among younger adults increase the risk for higher rates of colorectal cancer in the future.
FOLLOWING SCREENING GUIDELINES CAN CATCH COLORECTAL CANCER EARLIER
Screening can potentially catch precancerous polyps as well as identify colorectal cancer in its early stages. The U.S. Preventive Services Task Force recommends colorectal cancer screening begin at age 50, but people with Crohn’s disease or other risk factors should be screened earlier. Several screening tests can be used. Among those screened in 2018, most BCBS commercially insured members had colonoscopies. Twenty-seven percent used Fecal Immunochemical Tests (FIT) and 13% used Fecal Occult Blood Tests (FOBT)
BCBS AXIS7 INDICATES THAT ONLY A SMALL NUMBER OF PATIENTS BETWEEN THE AGES OF 50-52 ARE GETTING COLORECTAL CANCER SCREENING.
Among the population 50 years and older, most are waiting well beyond their 53rd birthday to begin colorectal cancer screening. BCBS Axis data show that between the ages of 50 and 52, only 30% of this population has been screened. The data also indicate these rates have not improved since 2016, remaining around 30% for ages 50-52.
For those under the age of 50 with Crohn’s or ulcerative colitis, 31% are getting screened in the preceding two years.8
DELAYED SCREENING COULD MISS CRITICAL WINDOW FOR EARLIER DIAGNOSIS
People who delay screening until their late 50s or early 60s are at risk of missing precancerous polyps or detecting colorectal cancer at an earlier stage. BCBS Health Index data indicate a 50% increase in colorectal cancer prevalence between ages 50 and 55
Rates of colorectal cancer screening vary nearly twofold across states, with rates being higher in the Northeast and lower in the Southwest .9 In addition, 15 states have colorectal cancer rates that are higher than the national average and screening rates that are lower than the national average.
ATTITUDES TOWARD COLORECTAL CANCER SCREENING
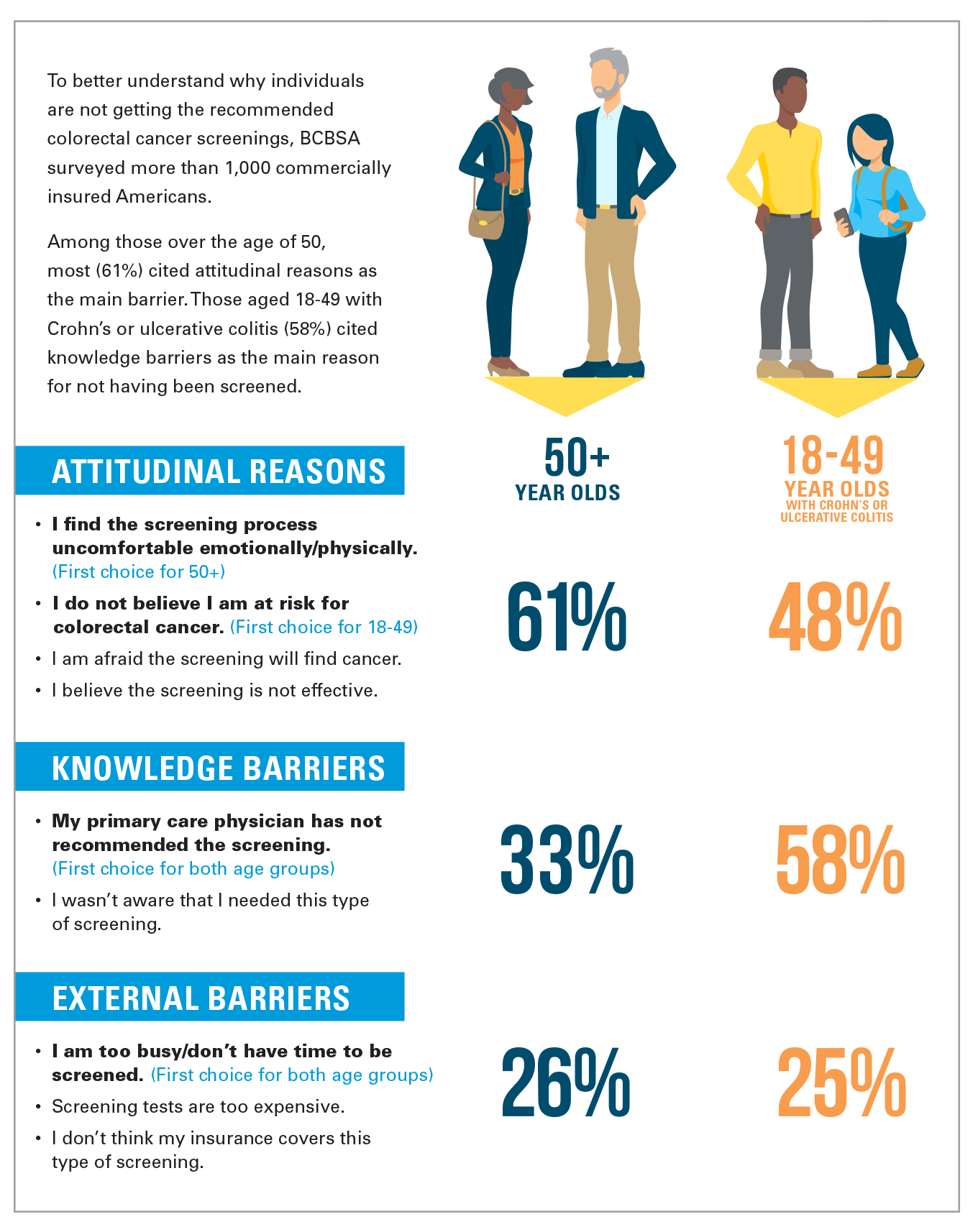
To better understand why individuals are not getting the recommended colorectal cancer screenings, BCBSA surveyed more than 1,000 commercially insured Americans. Among those over the age of 50, most (61%) cited attitudinal reasons as the main barrier. Those aged 18-49 with Crohn’s or ulcerative colitis (58%) cited knowledge barriers as the main reason for not having been screened.
ATTITUDINAL REASONS
- I find the screening process uncomfortable emotionally/physically. (First choice for 50+)
- I do not believe I am at risk for colorectal cancer. (First choice for 18-49)
- I am afraid the screening will find cancer.
- I believe the screening is not effective.
18-49 YEAR OLDS WITH CROHN’S OR ULCERATIVE COLITIS: 48%
KNOWLEDGE BARRIERS
- My primary care physician has not recommended the screening. (First choice for both age groups)
- I wasn’t aware that I needed this type of screening.
18-49 YEAR OLDS WITH CROHN’S OR ULCERATIVE COLITIS: 58%
EXTERNAL BARRIERS
- I am too busy/don’t have time to be screened. (First choice for both age groups)
- Screening tests are too expensive.
- I don’t think my insurance covers this type of screening.
18-49 YEAR OLDS WITH CROHN’S OR ULCERATIVE COLITIS: 25%
A CALL TO ACTION
People at highest risk for colorectal cancer, including those over the age of 50 and especially those with diagnoses of Crohn’s and ulcerative colitis, diagnosed obesity or diabetes have an opportunity to prevent and catch the disease earlier by receiving the recommended screening. Colorectal cancer prevalence rates increase by 50% from age 50-55, indicating that delaying screening by just a few years can have an impact. Understanding the risks of and managing chronic diseases can also play a significant role in reducing the impact of colorectal cancers. Doctors and patients, working together, can identify the appropriate timing and frequency of screening to reduce the burden of colorectal cancer.
METHODOLOGY
This is the 32nd study of the Blue Cross Blue Shield, The Health of America Report® series, a collaboration between Blue Cross Blue Shield Association and Blue Health Intelligence (BHI), which uses a market-leading claims database to uncover key trends and insights in healthcare affordability and access to care.
This report leverages data from three sources 1) BCBS Axis Data 2) the BCBS Health Index; and 3) a 2020 BCBSA consumer survey. The survey was self-reported from February 10-11, 2020 and consisted of commercially insured individuals ages 18- 49 (n=643) or age 50+ (n=497).
The prevalence rates were estimated using BCBS Health Index data between the years 2014-2018. This includes the rates of screening for the 50-52 year old population. Screening rates by age 52 were estimated by selecting those who were 52 in 2018. Colorectal cancer screening was then cumulative for these individuals in 2016, 2017, and 2018. Lifetime screening rates were self-reported through the 2020 BCBSA survey.
Increased risk of colorectal cancer was assessed by identifying 2 groups: People with Health Index data that had Crohn’s or ulcerative colitis in 2017 and people who did not. We then reduced this base population to those who had no diagnosis of colorectal cancer in 2017. The rates of new colorectal cancer diagnoses in 2018 were estimated for the Crohn’s/ulcerative colitis population and the population without. The rates were then measured in a ratio of new colorectal cancer diagnoses for the Crohn’s/ulcerative colitis population vs. the population without Crohn’s/ulcerative colitis. This was subsequently done, replacing Crohn’s/ulcerative colitis with diabetes, and then diagnosed obesity. Rates of new colorectal cancer diagnoses in 2018 are represented, along with their rate ratios.
Original source can be found here.
Source: Blue Cross Blue Shield of Arizona





 Alerts Sign-up
Alerts Sign-up